
INTRODUCTION
The United States Food and Drug Administration approved the da Vinci Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA, USA) for gynecologic disease in 2005 based on evidence of safety and efficacy in hysterectomy at the University of Michigan [1]. In Korea, the da Vinci system was first approved in July 2005, and the number of gynecological robotic surgeries has increased rapidly [2]. The adoption of robotic procedures to perform gynecological surgeries, particularly hysterectomies, was much faster than that observed with the adoption of laparoscopic procedures [3].
Hysterectomy is one of the most common gynecologic surgeries and has gradually developed over the years to provide minimally invasive surgery for women. The American Association of Gynecologic Laparoscopists recommended that most hysterectomies for benign diseases should be performed vaginally or laparoscopically [4]. Previous studies have shown that robotic hysterectomy is a minimally invasive, safe, and effective alternative to the conventional laparoscopic surgery. Clinical outcomes, such as smaller incision, less postoperative pain, blood loss, hospital safety, and complications in robotic hysterectomy, are similar to those in conventional laparoscopic hysterectomy [3,5].
Robotic approach has significant advantages in hysterectomy [6]. Although there is a lack of haptic feedback and direct access to patients, magnified three-dimensional vision is beneficial during surgery in difficult cases of hysterectomy [7,8]. Additionally, robotic instruments have a special function, with the EndoWrist® technology providing precise movement and enhanced exposure. EndoWrist® technology allows advanced laparoscopic techniques with a rapid learning curve for difficult tasks, such as intracorporeal suturing and knot-tying. The use of an articulated robotic instrument can be of great benefit when surgeons face a large uterus or dense adhesions during hysterectomy.
The da Vinci systems in robotic surgery have been serially developed into various types, including S, Si, X, and Xi. The new da Vinci Xi system was developed in 2014, and it overcomes several limitations of the previous da Vinci Si system. The da Vinci Xi shows greater vision and supports the scope of all four robotic arms to expand the visualization of anatomy. The da Vinci Xi system has a wider range of motion with thinner arms [9-11]. It does not require calibration, draping, or white balance, and ensures easier and faster docking. With the development of various da Vinci systems and expansion of the application of robotic surgery for gynecological diseases, robotic surgical platforms and instruments used in robotic hysterectomy have become very diverse. The number and location of ports can vary, depending on the uterine size, procedure (need to perform lymph node dissection), da Vinci system, and surgeonŌĆÖs preference. In this review, we discussed the procedures of robotic hysterectomy, with a focus on different surgical platforms and instruments in the da Vinci Xi system.
BASIC SYSTEMS OF THE da VINCI®
Robotic systems consist of three major components [12]: the surgeon console, where the surgeon sits and remotely controls the operating field using a stereoscopic viewer, hand manipulators, and foot pedals. Movements at this console are translated into movement of the surgical instruments at the operation site. The second component is a vision system that provides three-dimensional stereoscopic imaging through a dual optical endoscope. The third component is the robotic platform, which includes a patient-side cart with EndoWrist® instruments (Intuitive Surgical, Inc.). This system has either three or four robotic arms. One arm applied the laparoscope, and the other two to three arms applied various EndoWrist® instruments.
ROBOTIC INSTRUMENTS
All instruments and accessories of the latest version, the da Vinci Xi, are compatible with the da Vinci X system [12].
8-mm EndoWrist® instruments
Various EndoWrist┬« instruments have been used for multiport robotic surgery using the da Vinci Xi instruments (Table 1). The EndoWrist┬« instruments have 8-mm diameter rigid shafts. The total length of the shaft was approximately 21 in (53 cm). These EndoWrist┬« instruments feature a wrist-like mechanism that allows 7┬░ of movement and 90┬░ of articulation. This unique function replicates the full range of motion of the surgeonŌĆÖs hand and eventually overcomes the limitations of the conventional laparoscopy.
There are various types of graspers. The correct shape of the grasper can be selected according to the intended site of operation. Three types of monopolar cautery instruments provide an electrocautery capability to cut and coagulate tissues. Robotic scissors are useful for precisely cutting adhesions and controlling hemostasis using monopolar energy. Robotic hooks are excellent for dividing flimsy tissue and dissecting surrounding structures. A robotic spatula causes superficial tissue desiccation over a wide area. Bipolar forceps have dual functions, both as bipolar electrocautery instruments and retractors. Maryland bipolar forceps and curved bipolar dissectors have narrower tips that are useful for cautery and dissection in narrow spaces, whereas fenestrated bipolar forceps and force bipolar forceps can hold onto tissue more stably, which is good for applying traction. Of the bipolar cautery instruments, force bipolar forceps have the greatest grip strength, which allows stable grasping of relatively thick tissues without letting them slip by. Moreover, a large range of motion and grip strength are helpful in applying traction and cauterization of uterine vessels during hysterectomy. However, these bipolar forceps lack the strength required to apply traction to the myoma. In robotic myomectomy, tenaculum forceps are useful for applying traction to a myoma. Tenaculum forceps can be used to pull myomas in various directions. It helps to secure a clear field of vision and allows easy myoma separation. There are four types of needle drivers, which are generally categorized according to the presence or absence of the ability to cut. Needle drivers have wristed articulation and they enable suturing at multiple angles. Needle drivers with cutting ability are convenient because scissors are not required when cutting after suturing. However, caution is warranted when using these drivers because once in a while, sutures may be cut unintentionally. Two types of scissors were used, and three different sizes of clip appliers were selected according to vessel thickness. The EndoWrist┬« suction irrigator can be controlled by the surgeonŌĆÖs console.
5-mm Single-Site® instruments
The Single-Site® instruments have semi-rigid shafts with a diameter of 5 mm. The total length of the shaft was approximately 20 in (50.8 cm). A list of the Single-Site® instruments is shown in Table 2. Fewer instruments are available for use in a single-site surgery than in a multiport robotic surgery. Four types of dissectors and graspers are available for use in the single-site robotic surgery. For electrocautery, one type of monopolar cautery hook and two types of bipolar forceps are used. In a single-site surgery, instrument movement inside the abdominal cavity becomes very restricted; however, the Maryland bipolar forceps can be useful because of the benefit of curves and narrow tips. There are two types of needle drivers, one of which is a wristed needle driver with a rotatable joint. Wristed needle drivers are limited in that they cannot provide sufficient force application; however, they are helpful when suturing because the direction of the needle can be controlled by the presence of a joint on the instrument. Additionally, there is one type of curved scissors, a clip applier, and suction irrigator in the Single-Site® instruments.
CONVENTIONAL ROBOTIC HYSTERECTOMY
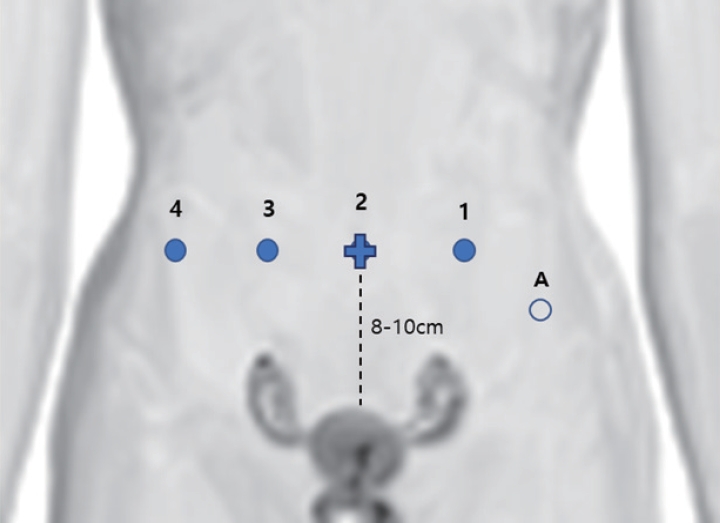
The conventional robotic hysterectomy procedure uses either four or five laparoscopic incisions (Fig. 1). The camera port location depends on the patientŌĆÖs height, uterine size, and surgical area [13]. For benign surgery, the 8-mm camera port should be placed 8-10 cm cephalic to the uterine fundus [14]. It is usually located at the umbilicus or 1-2 cm above the umbilicus. For oncologic surgery, the camera port is placed 20-25 cm above the pubic bone [15]. Care should be taken not to obscure the anatomical view by placing the camera port too close to the uterus or the pelvic mass. Under direct vision, two or three 8-mm trocars were placed 8-10 cm laterally from the umbilicus (on the left and right sides) to allow triangulation and prevent arm collision. Three 8-mm ports and the main assistant port were placed symmetrically in the upper abdomen. If required, an additional port for a bedside assistant is placed 2-3 cm below the left rib cage over the mid-clavicular line (Palmer point) or iliac fossa in the lower quadrants [16]. Surgeons can generally operate using monopolar instruments in the right operative arm, bipolar forceps in the left robotic arm, and a grasper in the rightmost port robot arm. The assistant can use suction/irrigation, suture material, instruments for retraction, and specimen removal through a 10- or 12-mm port [13].
THREE-PORT ROBOTIC HYSTERECTOMY
Experienced laparoscopic surgeons have attempted to reduce the costs and maintain efficiency by reducing the number of robotic arms. Additionally, fewer and smaller abdominal incisions increase patient satisfaction and reduce pain [17]. A previous study reported the safety and feasibility of the three-port robot-assisted hysterectomy technique [18]. This technique consists of three 8-mm trocars: one port on the umbilicus for a 0┬░ or 30┬░ optic and two lateral 8-mm ports for the instruments [18,19]. A 30┬░ optic can be useful in cases that allow access to uterine arteries and vesicovaginal fold or culdotomy in some cases with large uteri. Suction and irrigation are usually performed by a bedside assistant through one of the 8-mm trocars after removing one of the robotic instruments.
SINGLE-SITE ROBOTIC HYSTERECTOMY
Laparoendoscopic single-site surgery (LESS) was developed to further reduce the morbidity associated with minimally invasive surgery. Since the da Vinci Single-Site platform was introduced, robotic LESS has emerged as a feasible and widely applicable, minimally invasive approach in gynecologic surgery [20]. Previous studies on total laparoscopic hysterectomy using the da Vinci Single-Site platform showed that single-site robotic hysterectomy is safe and feasible, particularly in appropriately selected patients [21-24].
Using the open Hasson technique, a 2.5-3 cm vertical incision was made on the umbilicus (Fig. 2A). A multichannel single port was placed, and the peritoneum was created. Two ports are for robotic instruments: one port holds a camera, and the last one is an assistant port. After the table was placed in the Trendelenburg position, an 8-mm port and 30┬░ robotic camera were introduced into the abdominal cavity [25]. Two curved cannulas and 5-mm semi-rigid single-site robotic instruments were introduced. In addition to these instruments, the assistant can use suction/irrigation, suture material, and instruments for retraction through the same port [26].
SINGLE-SITE PLUS ONE OR TWO-PORT PLATFORM
Single-site robotic surgery has several limitations, including limited instrument clashing, reduced extracorporeal triangulation, and electrosurgical options, compared with conventional multiport robotic surgery. Additionally, this technique is not ergonomically friendly. To overcome these constraints, a single-site plus additional port platform is a challenging and feasible procedure in gynecological surgery [27,28]. This modified platform reduces the number of incisions, while maintaining the advantages of conventional robotic hysterectomy. After inserting a multichannel port into the umbilicus in the same way as the single-site platform, one or two additional 8-mm robotic trocars were placed in the lateral umbilicus, different from the singlesite port (Fig. 2B). Single-site robotic hysterectomy has inherent technical problems, including limited traction power with semi-rigid instruments and range-of-motion limitations [29]. An additional 8-mm robotic trocar compensates for this limitation and the EndoWrist® monopolar curved scissors were used through this additional port.
CONCLUSION
Robotic surgery enables gynecological surgeons to provide a more precise, safe, and minimally invasive approach for patients. Robotic surgery will continue to evolve as new surgical platforms and instruments are upgraded, alongside the development of robotic technology. Understanding the characteristics of various surgical platforms and instruments and selecting appropriate instruments and surgical platforms according to each patient for efficient surgery may help improve surgical outcomes.