
INTRODUCTION
Gynecoloogical surgeries for noncancerous conditions, such as hysterectomy or myomectomy by a minimally invasive approach has undisputed advantages compared to abdominal approach. Still 30.2% of hysterectomy is approached by abdominal route [1]. In a web based survey in UK gynecologists open myomectomy was the procedure performed by 74% respondents [2]. Committee opinion published in 2020 by American College of obstetricians and Gynecologists as well as Society of Gynecological Surgeons recommended that robot-assisted gynecologic surgery can be performed safely in centres with experienced surgeons and has perioperative outcomes equivalent to laparoscopy and improved outcomes compared with laparotomy [3]. This can reduce the need for abdominal approach especially in complex conditions as an alternative surgical tool.
Robot-assisted surgery has grown exponentially since the U.S. Food and Drug Administration (FDA) approved its use for gynecological surgery in 2005. Most studies reported in literature are retrospective, observational, and noncomparative. When compared to laparoscopic surgery, lowquality evidence suggests little difference in complication rates [4]. Although most studies report a longer operating time and cost with robotic surgery. The operating time improves rapidly with the learning curve followed by docking time and suturing durations [5]. The aim of the study was to analyze our experiences single centre, single surgeon experience with Davinci Si system over a period of 10 years.
MATERIALS AND METHODS
A total of 452 patients who underwent a robotic gynaecological operation at a tertiary hospital between August 2012 to July 2021. The Institutional Ethics Committee-Biomedical Research, Apollo Hospitals, Hyderabad (IEC No. AHJ-ACD-045/04-21) approved of the study. Da Vinci Si system was used during this period. The hospital upgraded to da Vinci Xi from August 2021, hence cases after this period were excluded from this study. This study was a retrospective chart review of a prospectively collected data. Demographic, previous medical conditions, previous abdominal surgery, pathology, intra operative and immediate postoperative course were reviewed. Demographic data included, parity, body mass index (BMI), previous history of abdominal surgery and the number of caesarean sections, and the surgical procedure as well as the indication for surgery. Docking and console time was recorded. Robot docking time (defined as time taken from the end of port placement to the time the surgeon began surgery at the console. Console time (defined as time surgeon spent sitting at the console and performing the operation). We also recorded clinical size of uterus, postoperative haemoglobin drop and blood transfusion. Additionally, cases with myomectomy recorded the number and location of myomas as well as the specimen weight. Any conversions to open surgery or additional procedure performed was recorded. Post operative data included the requirement of intra venous (IV) analgesia (hours), length of stay (LOS), blood transfusion. The number of robotic and assistant ports were noted in all cases.
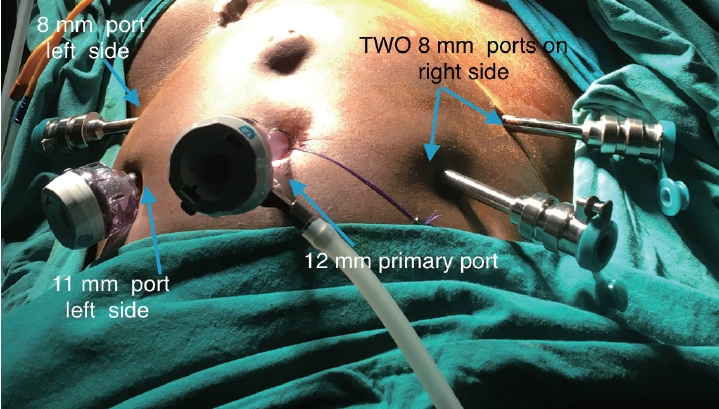
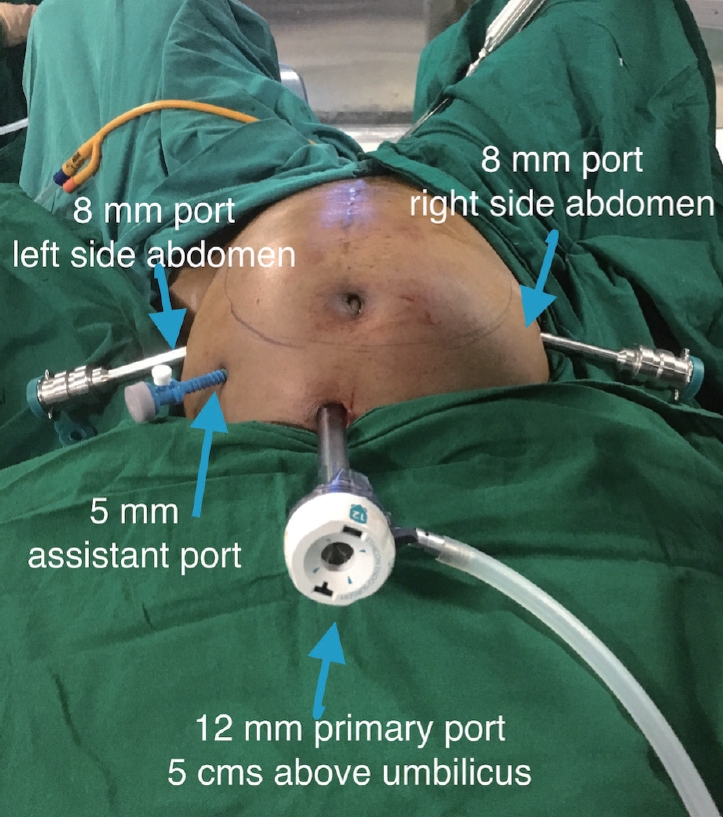
All patients underwent robotic surgery under general anaesthesia in a dorsal lithotomy position. A primary port (12 mm, XL trocar; Ethicon Endo-Surgery, Somerville, NJ, USA) was either placed at the umbilicus or at the Lee Huang point. Three secondary (8 mm; Intuitive Surgical, Inc., Sunnyvale, CA, USA) ports were used, two on the right side of the patient and one on the left side of the patient. The 11-mm assistant port was used on the left side of the patient (Fig. 1). The patient cart was placed parallel to the operation table on the right side (Fig. 2). Hot shears and the prograsp/tenaculum on the right side with the fenestrated bipolar in left port. At suturing the hot shears was replaced with mega needle driver. After the 27th cases we did not use the third robotic arm for our surgeries any more. This step reduced the need for one extra instrument, reducing the cost as well as the reduced the external arms clash. Two robotic secondary ports (8 mm) were placed laterally, one on the right side of the abdomen and one 8-mm on the left side of the abdomen and one 5-mm assistant port on the right side above the 8-mm port at 8-10 cm lateral to midline and 3-4 cm inferior to the optic trocar. A line was then drawn from the left 8-mm trocar and the optic trocar. At the mid-point of this line, a perpendicular line was drawn in the cranial direction and a 5-mm assistant port was placed at 4-5 cm from the line (Fig. 3). All cases were performed with 30-degree telescope. Hot shears on the right side with the fenestrated bipolar in left port. At suturing the hot shears was replaced with mega needle driver.
Data entry was done using M.S. Excel and it was statistically analyzed using statistical package for social sciences (SPSS) version 26 for M.S. Windows 2010 (IBM, Chicago, IL, USA). Descriptive statistical analysis was carried out to explore the distribution of several categorical and quantitative variables. Categorical variables were summarized with number (%), while quantitative variables were summarized by mean±standard deviation. All results were also presented in tabular form and are also shown graphically using bar diagram or pie diagram as appropriate. Inferential statistics: the difference in the two groups were tested for statistical significance using parametric tests such as t-test and analysis of variance (ANOVA) test. Categorical variables tested by chi-squared test. P-value less than 0.05 considered to be statistically significant.
RESULT
A total of 452 patients were included in the study period. The analysis was performed on 434 patients who fell in to three broad categories of indication for performing robotic surgery, namely myomectomy (n=204), hysterectomy (n=150) and endometriosis excision (n=80). The other patient underwent surgeries in this time period were: repair of genito urinary fistula (n=3), sacrocolpopexy for post hysterectomy prolapse (n=2), ovarian cystectomy (n=11), ectopic pregnancy (n=2). The mean age of patients in this study was 38.25±8.40 years. The mean age in robotic hysterectomy (RH) group was 46.12±6.77 while in robotic myomectomy (RM) was 34.14±5.50 and robotic endometriosis (RE) group was 34.16±6.69. The mean age in RH is high when compared to RM and RE which is statistically significant in ANOVA test (Table 1).
The mean BMI was 28.89±5.02 kg/m2 in this study population. Mean BMI in RH is high compared to RM and RE and this difference is statistically significant in ANOVA test (Table 1). The indications for RH were fibroid (n=76; 50.67%), adenomyosis (n=40; 26.67%), endometrial hyperplasia (n=20; 13.34%), endometriosis (n=10; 6.67%), and large multiple fibroids (n=6; 4%). In the RM group the indication for surgery were heavy menstrual bleeding in (n=156; 76.47%), dysmenorrhea in (n=133; 65.2%), mass (n=25; 12.17%), and frequency of urine (n=1; 0.4%). In fact, the commonest indication for doing robotic surgery in our series was fibroid uterus (288 cases; 63.7%).
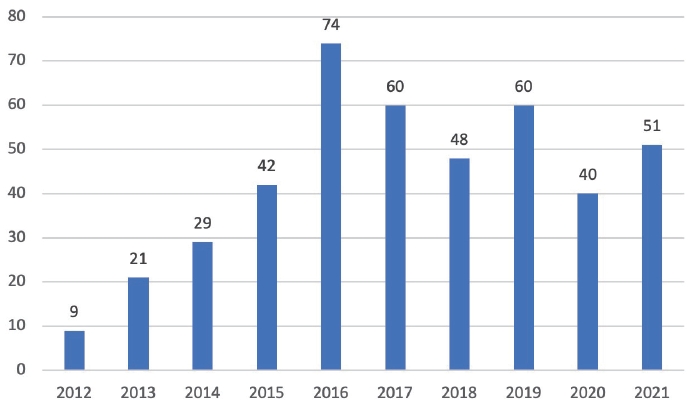
The number of cases done by robotic surgery increased over the years. We started our robotic program in August 2012 and did nine cases in that year, while in 2021, the last year of our analysis we did 51 cases.
The mean docking time over 10 years was 10.59±5.57 minutes. The docking time steadily reduced over the years as the case volume increased as shown in Fig. 4. The mean docking time in beginning of the learning curve in 2012 was 27.78 minutes which improved to 7.04 minutes in 2021 (Fig. 5). However, we reached the sweet spot of 8.33 minutes in docking time by 175th case after 5 years of robotic surgery at our hospital. When the docking is compared between the different surgeries it is seen high in RH group when compared to RM and RE and this difference is statistically significant in Kruskal-Wallis test.
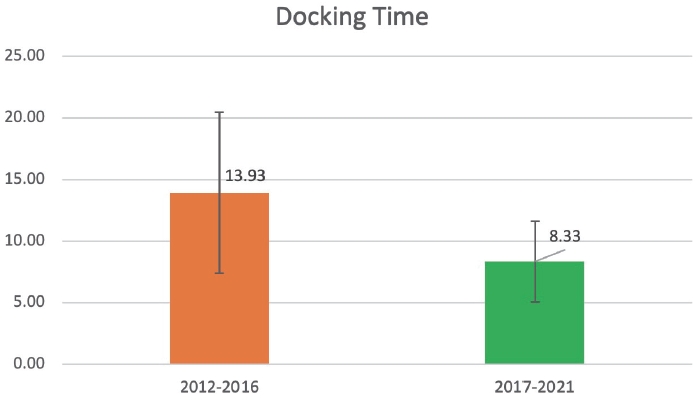
When we analysed our docking time in the first 5 years (2012-2016; n=175) and the last 5 years (2021-2016; n=279) there was a significant difference (P=0.0001). The first 5 years the average docking time was 13.93±6.15 minutes and the last 5 years (2017-2021) was 8.33±3.27 (Fig. 6).
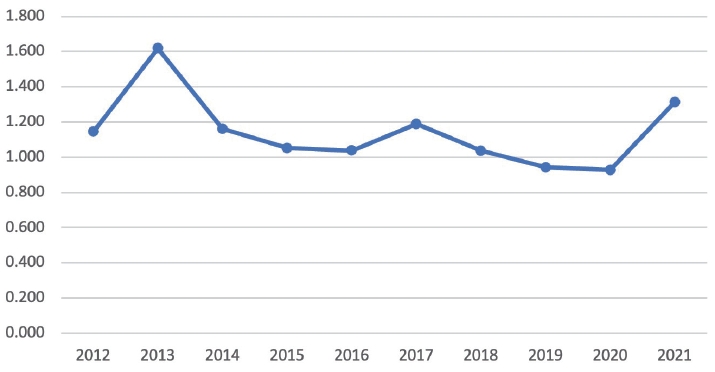
The console time averaged as 96.35±47.7 minutes. The analysis of the console time between the first 5 years and the last 5 years also showed significant difference (P=0.001). The mean console time in first 5 years was 105.74±52.44 and the last 5 years was 89.97±43.28 (Fig. 7). The mean console time in beginning of the learning curve in 2012 was 118.33 minutes which improved to 94.24 minutes in 2021 as shown in Fig. 7.
When the console time is compared between the different surgeries it was found to be high in RM compared to RH and RE and this difference was statistically significant in Kruskal-Wallis test.
The mean hemoglobin drop in all patient was 1.109± 0.7531 g% (Fig. 8). The drop of hemoglobin in individual groups were RM (1.30±0.84), RH (0.95±0.69), and RE (0.91±0.47). Mean hemoglobin drop was high in RM compared to RH and RE and this difference was statistically significant in ANOVA test (Table 1).
Ninety-three patients did not need any IV analgesia once they were shifted out of operating room (OR). Fifty-two patients required a dose in next 24 hours and only five patients stayed back for pain management by IV analgesia after 24 hours.
86.6% had less than 24 hours of LOS and 13.4% patients stayed more than 24 hours but none beyond 72 hours. We had one case of readmission who presented as a port site hernia after RH and needed exploration with end-to-end anastomosis [6]. There was no urinary tract injury in this series. However, one case has a rectal injury in RH group with grade 4 endometriosis, detected and repaired intraoperatively.
The mean specimen weight of leiomyoma in RM group was 323.8 g (200–1,372 g) and multiple leiomyomas were noted in 84 cases. Two cases of RM had intraoperative strategic conversion. One case had dense adhesions due to midline scar of previous myomectomy and the other had a deep seated myoma in lower uterine segment extending into left fornix. Enucleation was extremely difficult in one case due to preoperative prolonged use of ulipristal acetate.
In RH cases, the average size of uterus was corresponded to clinical size of 14 weeks (12–28 weeks). The specimen was retrieved by vaginal cold knife morcellation in 96.6% however, five patients had limited vaginal space with large specimen underwent morcellation through umbilical port using Xcite technique [7]. Two patients required suprapubic incision towards the end of the procedure. One due to presence of a large cervical fibroid with dense bladder adhesions due previous two lower segment cesarean section and another due to excessive hemorrhage. The cases with RE 40% patients had stage IV endometriosis and 53.75% had stage III endometriosis (revised American Society for Reproductive Medicine). We had an intraoperative complication of rectal serosal injury in one patient with stage 1V endometriosis with dense adhesions, which was managed by intracorporeal repair.
Post-operative complications were recorded according to Clavien dindo classification. One patient had grade I complication of paralytic ileus managed conservatively. Grade II complication involving blood transfusion was noted in 12 patients (RM), 13 (RH) and in one RE group.
DISCUSSION
U.S. FDA approved the use of robots for gynecological surgery in 2005. Although increased cost has been the reason cited for slow adoption of robotic surgery, the benefits of improved ergonomics and advanced instrumentation are becoming increasingly important considerations for surgeons to include this in their surgical practice. Its application in management of both benign and malignant conditions has steady increased. In a review by Truong et al. [8], the authors discuss that robotic assistance is utilized for hysterectomies, myomectomy, endometriosis surgery, sacrocolpopexy, adnexal surgery, tubal re-anastomosis, and cerclage. These are similar indications for which we have used the robotic assistance. We present a single surgeon, single centre experience in benign gynecology over 10 years. The three commonly performed procedures for benign gynecology were included to analyse the trends and the progress over 10 years using the da Vinci Si system.
The adoption of robotic surgery in benign gynecology has been slow but steady. In the period 2005–2013, abdominal hysterectomy declined from 59% to 22% according to premier perspective database [9] and by 2012 the hysterectomies performed by minimally invasive surgery rose to 75% [10]. This was associated with parallel increase in RH which increased from 26% to 61% and the same study and showed that high-volume surgeons were more efficient and showed a decrease in OR time after 75 cases despite an increase in uterine weight [11].
Laparotomy remains the most common method of doing myomectomy. Dallas and colleagues reported that since 2012 there is an increasing number of myomectomies performed minimally invasively, with a corresponding decrease in abdominal myomectomies and suggested that myomectomy via robot is one of the main reason for this shift [12]. Myomectomy is a suture intensive surgery and wristed instruments can mimic suturing as in open surgery and can help surgeons suture with much more ease. The mean age of patients in this study was 38.25±8.40 years. However, the mean age in RH was statistically high when compared to RM and RE. This reflection of the fact that myomectomy and endometriosis excision surgery is done for young women wanting to preserve their fertility. BMI was higher in RH cases. The author is skilled at total laparoscopic hysterectomy (TLH) and thus the cases that were selected for RH were with complexity multipliers like obesity, larger uterine volume, advanced endometriosis which are technically difficult TLH. The idea was to reduce intra operative conversions in cases of difficult TLH to minimal access surgery.
The mean age and mean BMI in the RH group was significantly higher as compared to RM and RE groups. One reason to offer hysterectomy by robotics was obesity in our clinical setting. The specific advantage of hysterectomy in obese women has been well established and the reduced chance of conversion to open surgery [13,14]. In fact, the authors have published their result of reducing the conversions from 10.9% to 4.3% in cases with large uterus [15]. In the present series 50% cases of RH were done for fibroid uterus and in fact, 63.7% of all cases in all groups were for fibroid uterus.
The robotic program at our centre started in 2012 and progressed slowly as it was new and expensive technology and was not covered by insurance at that time and also the author was already a skilled laparoscopic surgeon. Hence the cases who were offered were with complex gynecological indications. Similarly Lim et al. [9] reported that complex comorbidities, such as severe adhesions, obesity, or deep infiltrating endometriosis, are well suited for robot-assisted surgery. The reduction in the numbers in 2020 and 2021 could be attributed to COVID pandemic as the elective cases reduced during this period. Gupta et al. [16] reported a 39% decrease in gynecological surgery from 2019 to 2020 with hysterectomy being the most commonly performed procedure, while surgery for endometriosis and uterine fibroids had the greatest decrease in volume.
Docking time in robotic surgery refers to the amount of time taken for the robotic arms to be positioned and attached to the ports before the surgeon can begin surgery at the console. Docking time has been a source of constant criticism for robotic surgery as it is attributed to the additional OR time in robotic surgeries [17]. This time can vary depending on the experience of the surgical team (OR staff and technicians) and the specific robotic system being used. Additionally, space limitations, inadequate room configuration, lack of specialized training, and inadequate team communication and coordination.
It is generally considered that an efficient OR will reduce the docking time to an average of 8 minutes, the so-called “sweet spot”. In our study we could reach this average in 5 years. The reasons for this are multiple. In the initial years, the team was not trained nor assigned for this role. The number of cases in all specialities including gynecology averaged 4-5 cases a month. In 2016 the hospital hired a trained robotic technician and assigned him the “leader”, identified separate nursing staff for the robotic OR and with consistent training the docking time was reduced.
Rajanbabu in her analysis of operating times over years has reported improvement of docking time from nearly 13 minutes in the first year to less than 3 minutes in the fifth year [18]. The longer time to decrease the docking time could also be due to using the da Vinci Si system as compared to da Vinci Xi system.
Console time is a reflection of the learning curve, complexity of the case, requirement of multispecialty efforts and the skill of the surgeon. We consistently improved the console time over years. However, the last 5 years showed a significant reduction in the console time in our study irrespective of the indication. The console time also reached a plateau after the first 3 years. Similar reports have been published in the literature as well. It has been described that as the surgeon becomes proficient in surgery the curve plateaus that is there is minimal improvement after a certain period [19].
Although the amount of hemoglobin drop (surrogate marker of blood loss) was low across all types of surgery, it is interesting to note in this paper that the loss was significantly more in RM group when compared to other two groups. This is reflection of the fact that myomectomies in general have higher blood loss due to constant oozing from the hysterotomy bed while the uterine reconstruction is being done. However, we have also published our result of comparisons bet RM and laparoscopic myomectomy (LM) where LM has more blood loss. We believe that the less time taken in suturing when robot is being used is responsible for this result. Patients in the RM group had significantly less blood loss (115.43±79.43 vs. 340.98±453.9 mL, P≤0.0001) and requirement of blood transfusion (93.97% vs. 81.97%, P=0.031) when compared to LM group [20]. Lim et al. [9] also reported significantly fewer patients in the robotic-assisted cohort required intra-operative blood trans-fusions compared with patients in the abdominal, vaginal, and laparoscopic cohorts.
In our analysis, 86.6% had less than 24 hours of stay. Similarly reported by Lim et al. [9], where the mean length of hospital stay was shorter for the robotic-assisted group (1.37 days) than the open (3.0 days), vaginal (1.9 days), and laparoscopic (1.7 days) groups. They did not report any case of intra-operative hemorrhage, nerve injury, foreign bodies left in the peritoneal cavity, mechanical failure, or medical accidents. We did have one readmission for port site hernia on day 4 post operative day [6].
It is hypothesized that the significant reductions in postoperative gastrointestinal, genitourinary, thromboembolic, and respiratory complications are attributable to the combination of the robotic technology with surgical experience and proficiency of the surgeon in doing minimal access gynecological surgery.
Strength of this study is a long duration of study period that included both the learning curve and the later years of proficiency of the surgeon. All cases were performed only on the da Vinci Si system so the bias between two system did not enter in this study analysis. The limitation is that it is a single centre, single surgeon study. The cases were selected individually which depended on the surgeon and patients’ choice and consent.
Adoption of robotic surgery for benign gynecologic surgery is on the rise and provides several technological advantages. It is feasible and safe. Both robotic and laparoscopic approaches have been demonstrated Equivalent perioperative outcomes for hysterectomy, myomectomy, sacrocolpopexy, and endometriosis surgery. Robot-assisted surgery has demonstrated superior perioperative outcomes compared with laparotomy. Improved clinical outcomes and significantly lower postoperative complications despite the complexity of patients being higher. Reductions in intra operative and postoperative complications could translate to reductions in the over-all economic burden of treatment, with reduced incidence of surgical or medical injury correction, shorter hospitalization, fewer repeat surgeries, shorter recovery with less pain, and less time lost from work or normal activities, with concurrent improvements in quality of life.